![]()
Vitorino Modesto dos Santos (1) Melissa Gebrim Ribeiro (2) Manoel da Costa Gondim Neto (2) Iara Machado Motta
![]()
(2) Manoela Fassina Barros (3) Barbara Assumpção Paes Leme (3)
![]()
This article is licensed un- der a Creative Commons Attribution – Non Com- mercial – No Derivatives
4.0 International Licence
![]()
Professor-adjunct of Internal Medicine; Internal Medicine Department of Armed Forces Hospital, Brasília-DF, Brazil. Catholic University of Brasília, Brasília-DF, Brazil.
Medical Resident, Armed Forces Hospital, Brasília- DF, Brazil. Catholic University Medical Course, Brasília-DF, Brazil.
Intern of Medical Course, Catholic University of Brasília, Brasília-DF, Brazil.
Correspondence:
Prof. Dr. Vitorino Modesto dos Santos. Armed Forces Hospital. Estrada do Contorno do Bos- que s/n, Cruzeiro Novo. 70658-900, Brasília-DF, Brazil. Phone: #55-61 39662103. Fax: #55-61
32331599
E-mail: vitorinomodesto@gmail.com
![]()
Recibido: 06 – November – 2014
Aceptado: 01 – December – 2014
![]()
Key words: Rheumatoid arthritis; Subclinical hypothyroidism; Yellow nail syndrome; Case report.
Context
The yellow nail syndrome is a scarcely reported condition, and its physiopathology is not well understood. The main characteristics of this syndrome are yellowish discoloration of the nail plates, pulmonary changes and pleural effusion, and lymphedema of the lower limbs.
Case Report
An 85-year-old Brazilian woman, with history of bronchial asthma, rheumatoid arthritis and arterial hypertension, was complaining of breathlessness, lower limb edema, and intense oliguria. Over the previous 40 years she had been treated with aurothioglucose, prednisone, and NSAIDs. Yellowish nail changes developed in her hand and toe fingers, and lung and pleural changes were detected by chest radiography and computerized tomography. With evidence of classical triad, the yellow nail syndrome was characterized. Laboratory tests showed elevated levels of TSH and normal levels of free-T4, establishing the additional diagnosis of subclinical hypothyroidism.
Conclusion
![]()
The purpose of this report is to discuss uncommon associated conditions with yellow nails syndrome, which is considered a rare clinical entity.
Cite this article as:
Santos VM, Ribeiro MG, Gondim Neto MC, Motta IM, Barros MF, Leme BAP. Elderly woman with yellow nail syndrome, rheumatoid arthritis and hypothyroidism. Rev Med Vozandes 2014; 25: 43 – 46
Palabras clave: Artritis reumatoide; Hipotiroidismo subclínico; Síndrome de las uñas amarillas; Reporte de caso

Contexto
El síndrome de las uñas amarillas es una condición escasamente reportada, y su fisiopatología no es bien entendida. Las principales características de este síndrome son la decoloración amarillenta de las placas de las uñas, alteraciones pulmonares y efusión pleural, y linfedema de las extremidades inferiores.
Presentación de caso
Mujer brasileña, 85 años de edad, con antecedentes de asma bronquial, artritis reumatoide y hipertensión arterial se quejaba de falta de aire, edema de miembros inferiores y oliguria intensa. Durante los últimos 40 años había sido tratada con aurotioglucosa, prednisona, y AINEs. Uñas amarillas desarrollaron en los dedos de manos y pies, y cambios pulmonares y pleurales fueron detec- tados por radiografía de tórax y tomografía computarizada. Con evidencia de la tríada clásica, se caracterizó el síndrome de las uñas amarillas. Las pruebas de laboratorio mostraron niveles elevados de TSH, con niveles normales de T4 libre, y se estableció el diagnóstico adicional de hipotiroidismo subclínico.
Conclusión
El propósito de este informe es analizar condiciones poco comunes asociadas con el síndrome de las uñas amarillas, que se considera una entidad clínica rara.

Figure 1. Gross features of extremities with typical deformities of chronic rheumatoid arthritis. Hand fingers with absence of lunulae, and nail dystro-
phy in the 3rd, 4th and 5th right fingers. Toe fingers showing more accentuated nail changes, which include dystrophic inspissation, yellowish discolo- ration; signs of onycholisis, and some excessive curvatures of pincer nails.
The yellow nail syndrome (YNS) has been considered rare, with unknown etiopathogenesis, and can be related to morphological and functional changes in lymphatic vessels [1-5]. YNS was des- cribed for the first time in 1964 by Samman and White [6], and is classically characterized by yellowish discolored nails, lower limb edema and pleural effusion [1-7]. However, two of these changes are sufficient to establish the diagnosis of this syndrome [7]. Diverse conditions can be associated with the YNS, as example of rheu- matoid arthritis, autoimmune thyroiditis, systemic lupus erythe- matosus, drug side-effects, AIDS, malignancy, obstructive sleep apnea, xanthogranulomatous pyelonephritis, nephrotic syndrome, hypogammaglobulinemia, hypoalbuminemia, hyperthyroidism and hypothyroidism [1-5, 7]. Bronchial asthma, bronchiectasis, rhi- nosinusitis, recurrent pneumonia and pleural effusion are more frequent respiratory changes [6, 7]; genetic predisposition may be other causal factor [7].
Nail changes occur in one or all fingers and toes – yellowish color, slow growth, thickening, increased convexity, transverse grooves, onycholysis, onychorrexis, paronychia, in addition to deficiency of cuticle and absence of lunula [1, 3, 6]. YNS is more frequent in females and often affects middle-aged individuals; although occur in people from birth to over 80 years [4, 5]. YNS associated with rheumatoid ar- thritis and subclinical hypothyroidism is here described, comparing findings with five previous reports of this syndrome which may be underreported.

Figure 2. A and B. Images of chest radiography showing dilated heart chambers and blunting of the left costodiaphragmatic recess due to pleu- ral effusion;
C and D. Computed tomography revealing se- veral parenchymal fibrous sequelae, and conspi- cuous right pleural thickening.
An 85-year-old Brazilian woman came to our hospital because of severe dyspnea, lower extremity edema and oliguria during three days. Dyspnea on moderate efforts began 20 years ago and worsened recently. Antecedent of arterial hypertension and rheumatoid arthritis for 40 years, osteoporosis for 20 years, cholelithiasis, and crises of bronchial asthma. She had utilized solganal-B oleosum, which is an oily suspension of aurothioglucose, organic compound containing 50% gold for intramuscular injection to control rheumatoid arthritis. Current use of medicines includes codeine and paracetamol, carvedilol, ASA, oral calcium, in addition to prednisone (20 mg daily), ipratropium bromide, and fenoterol hydrobromide.
On physical examination, BMI: 25.9 kg/m², well oriented, hydrated, without cyanosis or jaundice, and afebrile; normal heart rate and heart sounds, absence of cardiac murmurs, jugular venous stasis at 45°; muffed breath sounds on the lung bases, diffuse bilateral crackles and wheezes; mixed edema in both lower limbs, and several bruises in all extremities. Besides classical deformities of rheumatoid arthritis, there were several hardened nodules in the following joints - metatarsal-phalangeal of the 1st and 2nd left toe fingers; metacarpal-phalangeal of the 2nd, 3rd and 5th right hand fingers and in the 2nd left hand finger; and proximal interphalangeal of the 3rd left hand finger. Moreover, there were dystrophic nails in both feet and in the 3rd, 4th and 5th right hand fingers; diverse inspissated nails with yellowish discoloration; some of them presenting onycholisis and onychorrhexis, in addition to accentuated transversal and longitudinal curvatures, which are classically indicative findings of pincer nails; figure 1.
Laboratory tests showed normal hemogram, pro-BNP: 11.483 (VR:
≤334) pg/mL, urea: 80.8 (VR: 16.6-48.5) mg/dL, creatinine: 0.9 (VR:
0.5-0.9) mg/dL, clearance of creatinine: 68 (VR: ≥60) mL/min, uric acid: 9.6 (VR: 2.4-5.7) mg/dL, triglyce- rides: 216 (VR: 150-200) mg/dL, potassium: 3.4 (VR:
3.5-5.1) mmol/L, TSH: 8.21 (VR: 0.27-5.0) mcUI/mL and
free-T4: 1.28 (VR: 0.93-1.7) ng/dL. The EKG revealed left branch block and enlarged left atrium. Transtho- racic echocardiogram showed ejection fraction: 24%, accentuated systolic disfunction of the left ventricle (LV), indeterminate diastolic dysfunction
of LV, moderate mitral insufficiency, and enlarged left atrium. Chest radiography showed globally enlarged heart area and lung congestion, in addition to blunting of the left costophrenic recess; computerized tomography revealed pleural and pa- renchyma sequelae in the right lung apex, atelectatic striae in right basal posterior segment, and ipsilateral pleural effusion; figure 2.
As the patient did not adhere to the recommended regular outpatient controls, her treatment could not be adequately oriented and the diagnoses of congestive heart failure and subclinical hypothyroidism were established during the admission at our hospital. She used enalapril, spironolactone, furosemide, alenia, oxycodone, and prednisone (7.5 mg daily). Initial suspicion of renal failure was ruled out with base in the clearance of creatinine; and the accentuated oliguria, which was claimed in hospital admission, was due to urinary reten- tion secondary to the adverse effect of longstanding abuse of codeine, which was withdrawn. The dose of glucocorticoid was gradually reduced and the patient was oriented about the correct posology of medicines. Currently, she is under rheuma- tology and cardiology outpatient care.
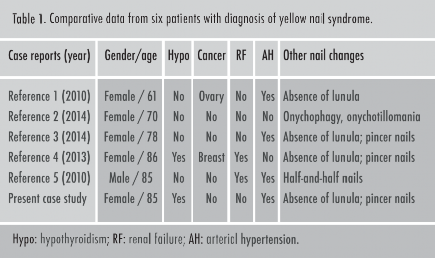
Comparative analysis of data from other five Brazilian case reports about YNS revealed 83.3% females, aged between 61 and 86 years, with median of 81.5 years and mean of
77.5 ± 10.1 years; arterial hypertension in 66.6%; renal failure in 33.3%; cancer in 33.3%; hypothyroidism in 33.3%; absence of lunula in 66.6%; pincer nails in 50%; and half-and-half nails and onycophagia in 16.6% each of the studied individuals; table 1.
Subclinical hypothyroidism. Worthy of mention in this case study is the association of YNS with rheumatoid arthritis plus this entity. A possible concern in the present setting might be about the role of symptomatic hypothyroidism as a risk factor of cardiovascular disease in elderly women with rheu- matoid arthritis [8]. McCoy et al evaluated a cohort of 650 patients with diagnosis of rheumatoid arthritis in comparison with equal number of controls; 69% were female, mean age
was 55.8 years [8]. Those authors concluded that symp- tomatic hypothyroidism has a significant association with cardiovascular disease in individuals presenting with rheumatoid arthritis, and plays a main role as contributive factor for morbidity and mortality in this group of chronic patients [8]. Subclinical hypothyroi- dism is a biochemical diagnosis characterized by persistently elevated levels of TSH, in concomitance with normal determinations of free-T4 [9-11]. Recently, this diagnosis has enhanced in frequency and occurs in 3% to 8% of population [10]. Worthy of note, is to re- member that physiological variations in TSH levels may occur with aging. Among people aged over 80 years the maximum normal levels of this hormone is 8 mcUI/L [11], whereas in the present case study the res- pective finding was beyond this limit. Therefore, the biochemical diagnosis of subclinical hypothyroidism was established [9-11].
Etiologic conditions of this syndrome include autoim- mune thyroiditis, subacute thyroiditis, postpartum thyroiditis, thyroid trauma, thyroidectomy, radioactive iodine, side-effects of drugs (amiodarone, lithium, interferon-alpha, ethionamide, sulfonamide, iron, carbonate of calcium, cholestyramine, phenobarbital, phenytoin, and carbamazepine), thyroid infiltration (amyloidosis, sarcoidosis, hemochromatosis, Riedel’s thyroiditis, SIDA, and lymphoma) and central hy- pothyroidism [11]. In some individuals the normalization of thyroid function may spontaneously occur; and the degree of elevation in the circulating levels of TSH constitutes the main prognostic factor [10]. Currently, there are scarce protocols for treatment of subclinical hypothyroidism in daily clinical practice. With TSH levels above 10 mcUI/L the effects are usually beneficial; but among the elderly group there is controversy if the levels are 4.5 to 10 mcUI/L, and results may be ad- verse [9-11]. Above the age of 80 years, the development of subclinical hypothyroidism could be considered to exert some protective cardiovascular effect [9].
YNS and rheumatoid arthritis. The first reference found about this rare association is from Sharvill in 1966 [12], in a case discussion of a patient with YNS, which was observed after treatment of the arthritis with a gold compound. Interes- tingly, after drug suspension the nail yellowish discolora- tion decreased in intensity and the nail growing returned to normal [13] The second reference is from Mattingly and Bossingham in 1979, reporting three cases of this association; however, only one of the patients, 59-years-old, utilized gold compounds [13]. Taki e Tobe also described the classic triad of YNS in a patient with gastric cancer and chronic rheumatoid arthritis, which was controlled by organic compounds of gold [14]. Mechanisms of the association between YNS and rheumatoid arthritis are totally cleared. Phenomena involved include the filtration ratio and capillary lymphatic clearance, abnormal immune responses, decreased IgA levels, immune deficiency, and drug adverse effect [13]. Accordingly with some of the case reports, a gradual reduction was observed in the intensity of yellowish nail discoloration over time after withdrawn of gold administration [13, 14].
YNS and hypothyroidism. Noël-Savina et al. (2012) reported typical YNS coexisting with symptomatic hypothyroidism and suggested a relationship between these conditions [15]. Santos et al. (2013), described the triad of YNS in an elderly woman with symptomatic hypothyroidism plus previous diagnosis of breast cancer and chronic renal failure [4]. Physiopathology mechanisms involved in this association remain to be entirely cleared; nevertheless, changes in microcirculatory regulation and slowing of blood capillary fluxes may be observed in the nail folds of individuals pre- senting symptomatic hypothyroidism [4].
Accordingly to literature YNS is a rare condition, but this entity may be underestimated. Descriptions of this syndrome in association with hypothyroidism have been very scarce. High index of suspicion regarding to the components of the syndrome, as well as thorough physical examination including evaluation of nail changes, could contribute to the diagnosis.
There are no conflicts to disclaim.
There was no grant support for this manuscript.
![]()
![]()
![]()
Santos VM, Marques HV Jr, Lima Cdo C, Tu- rra TZ, de Melo Jr Nogueira PR, Lima LN. Ye- llow nail syndrome and adnexal tumour:
causal or casual association? Indian J 6.
Chest Dis Allied Sci 2010; 52: 51-53.
Santos VM, Araújo MCM, Almeida ACA, 7. Brito KRA, Fachinelli LR, Mussi P. Onico- fagia, onicotilomania y síndrome de las uñas amarillas en mujer de 70 años. Pren Med Argent 2013; 99: 684-91.
8.
Santos VM, Blanger V, Cançado ACV, Carvalho MRM, Araújo MCM, Silva RF. Ido- sa com síndrome das unhas amarelas e unhas em pinça. Rev Med Saude Brasilia 2014; 3: 125-30.
9.
Santos VM, Ribeiro KRA, Santos AMRO, Nascimento ALO, Fachinelli LR, Caval- canti GF. Síndrome das unhas amarelas
gic patient with renal failure. Brasilia Med 2010; 47: 364-67.
Samman PD, White WF. The “yellow nail syndrome”. Br J Dermatol 1964; 76: 153-57.
Maldonado F, Tazelaar HD, Wang CW, Ryu JH. Yellow nail syndrome: analysis of 41 consecutive patients. Chest 2008; 134:
375-81.
McCoy Sara, Crowson CS, Gabriel SE, Matteson EL. Hypothyroidism as a risk fac- tor for development of cardiovascular di- sease in patients with rheumatoid arthritis. J Rheumatol 2012; 39: 954-58.
Fatourechi V. Subclinical hypothyroidism: an update for primary care physicians. Mayo Clin Proc 2009; 84: 65-71.
Raza SA, Mahmood N. Subclinical hy- pothyroidism: controversies to consensus. Indian J Endocrinol Metabol 2013; 17: 5636-42.
Sharvill DE. In discussion: Yellow nail syn- drome with bilateral bronchiectasis. Proc R Soc Med 1966; 59: 448.
Mattingly PC, Bossingham DH. Yellow nail syndrome in rheumatoid arthritis: report of three cases. Ann Rheum Dis 1979; 38: 475- 78.
Taki H, Tobe K. Yellow nail syndrome as- sociated with rheumatoid arthritis, thiol- compound therapy and early gastric cancer. BMJ Case Rep Mar 20; 2012. doi: 10.1136/bcr.11.2011.5183.
Noël-Savina E, Paleiron N, Leroyer R,
em idosa com hipotireoidismo: relato de caso. Brasilia Med 2013; 50: 342-45.
5. Santos VM, Sá DAR, Paz BCS, Vasconcelos RA, Santos SC, Santos FHB. Half-and-half nails and yellow nail syndrome in hemiple-
10. Lee MW, Shin DY, Kim KJ, Hwang S, Lee
EJ. The biochemical prognostic factors of subclinical hypothyroidism. Endocrinol Metabol (Seoul) 2014; 29: 154-62.
Descourt R. Découverte d’un syndrome
dês ongles jaunes lors d’une insuffisance thyroidïenne majeure. Rev Pneumol Clin 2012; 68: 315-17.